

Fast Facts
- SLE affects 10 times as many women as men
- Treatment depends on the type and severity of symptoms you experience
- Given its complex nature, treating SLE is often a team effort by several types of specialists and your own active participation in maintaining your health
What is SLE?
Systemic lupus erythematosus (also called SLE or lupus) is a chronic inflammatory disease of an autoimmune nature that can affect the skin, joints, kidneys, lungs, nervous system, and/or other organs of the body. The word “systemic” means the disease can affect many parts of the body, while “lupus” is the Latin word for “wolf” (so called because a French doctor in the 19th century likened the facial rash to the bites of a wolf).
The most common symptoms include skin rashes and arthritis, often accompanied by fatigue and fever. The clinical course of SLE varies from mild to severe, and typically involves alternating periods of remission and relapse.
There are several kinds of lupus:
- Systemic lupus erythematosus (SLE) is the one that most people refer to when they say “lupus”. The symptoms of SLE may be mild or serious. Although SLE usually first affects people between the ages of 15 and 45, it can occur in childhood or later in life as well.
- Discoid lupus erythematosus (DLE) is a chronic skin disorder in which a red, raised rash appears on the face, scalp, or elsewhere. The raised areas may become thick and scaly and may cause scarring. The rash may last for days or years and may recur. A small percentage of people with discoid lupus have or develop SLE later.
- Neonatal lupus is a rare disorder that can occur in newborn babies. Scientists suspect that neonatal lupus is caused by auto-antibodies in the mother’s blood called anti-Ro (SSA) and anti-La (SSB). Auto-antibodies (“auto” means “self”) are blood proteins that act against the body’s own parts. At birth, the babies have a skin rash, liver problems, and low blood counts. These symptoms gradually go away over several months, although in rare cases, babies with neonatal lupus may have a heart problem that slows down the natural rhythm of the heart.
Some drugs may cause SLE-like features and hence this condition is called “drug-induced lupus”. The features typically go away completely when the drug is stopped. The kidneys and brain are rarely involved.
Who Gets SLE?
About 90 percent of people with SLE are women; the other 10 percent being men and children. SLE in women commonly begins in the childbearing years, and rarely in childhood and after menopause.
Because symptoms vary widely and SLE can show up in so many ways, it is difficult to be sure how common the disease really is. It is estimated that one person in 2,000 in the USA and one in 250 in Jamaica have SLE. So far, Malaysia does not have any nationwide statistics.
It has also been found that in the USA, SLE is three times more common in African American women than in Caucasian women, and is also more common in women of Hispanic, Asian, and Native American descent. In addition, SLE can run in families, but the risk that a child or a brother or sister of a patient will also have SLE is very low.
What Causes SLE?
SLE is an autoimmune disorder that develops when the body’s immune system begins to attack its own tissues. Its cause is unknown, but it is likely that a combination of genetic, environmental, and, possibly, hormonal factors work together to cause SLE. This occurs through the production of “auto-antibodies” that attack a person’s own cells thus contributing to the inflammation of various parts of the body, and may cause damage to organs and tissues.
The most common type of auto-antibody that develops in people with SLE is called an antinuclear antibody (ANA) because it reacts with parts of the cell’s nucleus (command centre). Scientists do not yet understand all of the factors that cause inflammation and tissue damage in SLE.
The fact that SLE can run in families indicates that its development has a genetic basis; however, no specific “lupus gene” has been identified yet.
Studies suggest that several different genes may be involved in determining a person’s likelihood of developing the disorder, which tissues and organs are affected, and the severity of disease. However, it is believed that genes alone do not determine who gets SLE and that other factors also play a role. Some of the other factors scientists are studying include sunlight, stress, certain drugs, and agents such as viruses.
What are the Symptoms?
Each patient has slightly different symptoms that can range from mild to severe and may come and go over time. However, some of the most common symptoms of SLE include painful or swollen joints (arthritis), unexplained fever, and extreme fatigue. A characteristic red skin rash – the “butterfly” or malar rash – may appear across the nose and cheeks. Rashes may also occur on the face and ears, upper arms, shoulders, chest, and hands. Because many people with SLE are sensitive to sunlight (called photosensitivity), skin rashes often first develop or worsen after sun exposure. Some people experience symptoms in many parts of their body. Just how seriously a body system is affected varies from person to person.
Typical clinical features include:
- Fever, fatigue, and weight loss
- Arthritis, involving multiple joints for several weeks
- Butterfly-shaped rash over the cheeks or other rashes
- Skin rash appearing in areas exposed to the sun
- Sores in the mouth or nose for more than a month
- Loss of hair, sometimes in spots or around the hairline
- Seizures, strokes and mental disorders
- Blood clots in different locations
- Miscarriages in some patients
- Blood or protein in the urine or tests that suggest poor kidney function
- Low blood counts (anaemia, low white blood cells or low platelets)
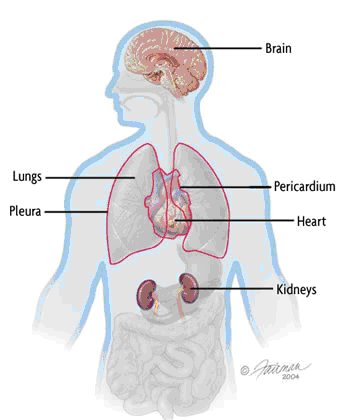
The following systems in the body can be affected by SLE
Kidneys
Inflammation of the kidneys (nephritis) can impair their ability to get rid of waste products and other toxins from the body effectively. There is usually no pain associated with kidney involvement, although some patients may notice swelling in their ankles. Most often, the only indication of kidney disease is an abnormal urine test or blood test. Because the kidneys are so important to overall health, intensive drug treatment is generally required to prevent permanent damage.
Lungs
Some people with SLE develop pleuritis, an inflammation of the lining of the chest cavity that causes chest pain, particularly with breathing. Patients may also get pneumonia.
Central nervous system
In some patients, SLE affects the brain or central nervous system. This can cause headaches, dizziness, memory disturbances, vision problems, seizures, stroke, or changes in behavior.
Blood vessels
Blood vessels may become inflamed (vasculitis), affecting the way blood circulates through the body. The inflammation may be mild and may not require treatment or may be severe and require immediate attention.
Blood
People with SLE may develop anaemia, leucopenia (a decreased number of white blood cells), or thrombocytopenia (a decrease in the number of platelets in the blood, which assist in clotting). Some people with SLE may have an increased risk for blood clots.
Heart
In some SLE patients, inflammation can occur in the heart itself (myocarditis and endocarditis) or the membrane that surrounds it (pericarditis), causing chest pains or other symptoms. SLE can also increase the risk of arteriosclerosis (hardening of the arteries).
How is SLE Diagnosed?
Diagnosing SLE can be difficult. It may take months or even years for doctors to piece together the symptoms to diagnose this complex disease accurately. Making a correct diagnosis of SLE requires knowledge and awareness on the part of the doctor and good communication on the part of the patient. The patient has to give the doctor a complete and accurate medical history (for example, what health problems he or she has had and for how long) as this is critical to the process of diagnosis. This information, along with a physical examination and the results of laboratory tests, helps the doctor consider other diseases that may mimic SLE, or determine if the patient truly has the disease. Reaching a diagnosis may take time as new symptoms appear.
No single test can determine whether a person has SLE, but several laboratory tests may help the doctor to make a diagnosis. The most useful tests identify certain auto-antibodies often present in the blood of people with SLE. For example, the antinuclear antibody (ANA) test is commonly used to look for auto-antibodies that react against components of the nucleus of the body’s cells. Most people with SLE test positive for ANA. However, there are a number of other causes of a positive ANA besides SLE, including infections and other autoimmune diseases. Occasionally, it is even found in healthy people
In addition, there are blood tests for individual types of auto-antibodies that are more specific to people with SLE – although not all SLE patients test positive for these and not all people with these antibodies have SLE. These antibodies include anti-DNA, anti-Sm, anti-RNP, anti-Ro (SSA), and anti-La (SSB). The doctor may use these antibody tests to help make a diagnosis of SLE.
Some tests are used less frequently but may be helpful if the cause of a person’s symptoms remains unclear. The doctor may order a biopsy of the skin or kidneys if those body systems are affected. Some doctors may order a test for anticardiolipin (or antiphospholipid) antibody. The presence of this antibody may indicate increased risk for blood clotting and increased risk for miscarriage in pregnant women with SLE. Again, all these tests merely serve as tools to give the doctor clues and information in making a diagnosis. The doctor will look at the entire picture – medical history, symptoms, and test results – to determine if a person has SLE.
Other laboratory tests are used to monitor the progress of the disease once it has been diagnosed. A complete blood count, urinalysis, blood chemistries, and the erythrocyte sedimentation rate (ESR) test can provide valuable information. Another common test measures the blood level of a group of substances called complement. People with SLE often have increased ESRs and low complement levels, especially during flares of the disease. X rays and other imaging tests can help doctors see the organs affected by SLE.
How is SLE Treated?
Management of SLE can be a challenge. Treatment depends on symptoms and their severity.
Treating SLE is often a team effort between the patient and several types of healthcare professionals namely, rheumatologists, nephrologists, haematologists, dermatologists, neurologists and psychiatrists. In treating a SLE patient, the doctor has to prevent flares, treat the flares, and minimise organ damage and complications.
The main medications are as follows:
NSAIDs
For people with joint or muscle pain, or fever, drugs that decrease inflammation, called nonsteroidal anti-inflammatory drugs (NSAIDs), are often used. NSAIDs may be used alone or in combination with other types of drugs to control pain, swelling, and fever.
Common side effects of NSAIDs can include stomach upset, heartburn, diarrhoea, and fluid retention.
Hydroxychloroquines
These anti-malarials are another type of drug commonly used to treat SLE. These drugs were originally used to treat malaria, but doctors have found that they are also useful for SLE. They may be used alone or in combination with other drugs and are generally used to treat fatigue, joint pain, skin rashes, and inflammation of the lungs. Clinical studies have found that continuous treatment with anti-malarials may prevent flares from recurring.
Side effects of anti-malarials can include stomach upset and, extremely rare, damage to the retina of the eye.
Corticosteroids
The main treatment in SLE involves the use of corticosteroids, the most common being prednisolone. Corticosteroids are related to cortisol, which is a natural anti-inflammatory hormone. They work by rapidly suppressing inflammation. Corticosteroids can be given by mouth, in creams applied to the skin, or by injection. Because they are potent drugs, the doctor will seek the lowest dose with the greatest benefit.
Short-term side effects of corticosteroids include swelling, increased appetite, and weight gain. These side effects generally stop when the drug is stopped. It is dangerous to stop taking corticosteroids suddenly, so it is very important that the doctor and patient work together in changing the corticosteroid dose.
Long-term side effects of corticosteroids can include weakened bones (osteoporosis), high blood pressure, high cholesterol, high blood sugar (diabetes), damage to the arteries, infections, and cataracts. The higher the dose and the longer they are taken, the greater the severity of side effects. Doctors try to limit or offset the use of corticosteroids. For example, corticosteroids may be used in combination with other, less potent drugs, or the doctor may try to slowly decrease the dose once the disease is under control. SLE patients who are using corticosteroids should talk to their doctors about taking supplemental calcium and vitamin D or other drugs to reduce the risk of osteoporosis.
Immunosuppressives
For some patients whose kidneys or central nervous systems are affected by SLE, a type of drug called an immunosuppressive may be used. Immunosuppressives, such as cyclophosphamide (Cytoxan) and mycophenolate mofetil (CellCept), restrain the overactive immune system by blocking the production of immune cells. These drugs may be given by mouth or by infusion (dripping the drug into the vein through a small tube). Side effects may include nausea, vomiting, hair loss, bladder problems, decreased fertility, and increased risk of cancer and infection. The risk for side effects increases with the length of treatment. As with other treatments for SLE, there is a risk of relapse after the immunosuppressives have been stopped.
The patient has to work closely with his or her doctor to help ensure that the treatments are as successful as possible. Because some treatments may cause harmful side effects, it is important for the patient to promptly report any new symptoms to the doctor. It is also important not to stop or change treatments without talking to the doctor first.
Quality of Life
While the treatment for SLE has improved and long-term survival has increased, it remains a chronic disease that can limit activities. More often, quality of life is compromised by symptoms like fatigue and joint pains, which are not life threatening. The best way to control SLE is to be very careful to take all your medications as prescribed, visit your physician regularly, and learn as much as you can about SLE, your medications, and your progress. Get involved in your care. Don’t take a back seat.
Despite the symptoms of SLE and the potential side-effects of treatment, patients can still maintain a high quality of life. One key to managing SLE is to understand the disorder and its impact. Learning to recognise the warning signs of a flare can help the patient take steps to ward it off or reduce its intensity.
Maintaining an active lifestyle will usually help keep joints flexible and may prevent cardiovascular complications. This does not mean overdoing it; the best approach is to alternate light to moderate exercise with periods of rest or relaxation.
Patients with lupus should avoid excessive sun exposure because the ultraviolet rays in sunlight can cause a skin rash to flare, and may even trigger a more serious flare in the disease itself. Wearing protective clothing (long sleeves, a big-brimmed hat) and using sunscreen liberally when outdoors on a sunny day should protect against such complications.
Staying healthy requires extra effort and care for people with SLE, so it becomes especially important to develop strategies for maintaining wellness. Wellness involves close attention to the body, mind, and spirit. One of the primary goals of wellness for people with SLE is coping with the stress of having a chronic disorder. Effective stress management varies from person to person. Some approaches that may help include exercise, relaxation techniques, and setting priorities for spending time and energy.
Developing and maintaining a good support system is also important. A support system may include family, friends, medical professionals, and support groups such as Persatuan SLE Malaysia.
Participating in a support group can provide emotional help, boost self-esteem and morale, and help develop or improve coping skills.
Learning more about SLE also helps. Studies have shown that patients who are well-informed and participate actively in their own care tend to experience less pain, make fewer visits to the doctor, and remain more active.